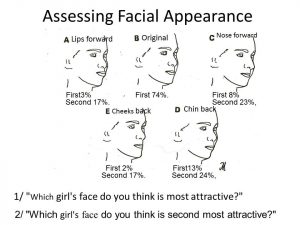
Facial appearance is hugely important for everyone’s success in life. Mothers often feel their child’s face is God given and should be accepted, however many teenagers are more concerned about their facial appearance than anything else. I have done a lot of research on facial form and in one project I traced the changes that I had achieved when treating a young girl and recorded them on a sheet of paper. I then reproduced the change of the lips, the nose, the cheeks and the chin separately and put them on a past board with the end result of all the changes in the centre. (See girl and tracings below).
I asked 106 lay people which face they preferred. The percentages are shown with the tracings and you can see that flat cheeks were by far the most unattractive feature. Interestingly receding jaws are not as big a drawback. Certainly those with forward growing cheeks and chins are considered far more attractive than anyone else.

In another project, I researched the judgements of lay people, dentists and orthodontists and was surprised to find orthodontists were less concerned about flat faces than the others. I wondered why that might be and found three other research papers had found the same thing, I suppose it is because orthodontists tends to flatten the face and they get used to a “straight profile”.
In another paper of mine Kieferorthopädie 2015;29(4):1–15, I collected 16 ‘Excellent’ results achieved by orthodontics and compared them with 16 ‘excellent’ results achieved by orthotropics. I was really surprised that twelve dental and lay judges found the faces and teeth of the orthotropics cases were “Highly Significantly” better than the orthodontic cases. When looking for reasons I think it must be the retruded and flattened cheeks created by fixed appliances.
John Mew has been working on a lecture series going into more depth on his thoughts, ideas and what inspired them. In this episode he talks about facial appearance, some research that he has undertaken and what make a face attractive.
If there are any other topics you want us to cover please let us know.
To engage with Prof John Mew or Dr Mike Mew on this topic;
Professionals (of any medical/health discipline); https://www.facebook.com/groups/Orthodont/ or https://www.facebook.com/groups/Orthodont/permalink/3397478746937698/
Non Professionals; https://www.facebook.com/groups/craniofacialactiongroup https://www.facebook.com/groups/craniofacialactiongroup/permalink/2971797196229944/
To see the text version please visit; https://orthotropics.com/john-mews-lectures-5-facial-aesthetics/
Please consider joining our Patreon Community: https://www.patreon.com/orthotropics
Particularly if you have;
1) gained any benefit from the information that we have provided (usually for free).
2) wish to have the benefits of being a patreon member.
3) believe in, and wish to support our mission to gain full, free and fair debate (engagement) on these issues within the orthodontic and dental community.
Best wishes,
Orthotropics Video Team.