Many clinicians from different disciplines offer explanations and cures for TMJ and it is widely assumed that there is no ‘One Size Fits All Treatment Guarantee’. However when part of the body goes wrong there is usually only one direct cause, although by coincidence two or possibly three causes could occur simultaneously. Most of the other factors are either, resultant, coincident, predisposing, or unrelated, but not causative. It is wise therefor to consider each one separately and then try to select the real culprit.
My research in anthropology convinced me that the jaw joints of our ancient ancestors rarely showed any signs of damage, so why does this joint cause so much trouble now? Things have changed since then and many jaw bones are now set back as much as 20 to 30mm from where they were back then. Most TMD clinicians agree that this distalization, causes pressure on the joint but there are few suggestions about how to improve it and surgery has not so far proved a reliable cure.
There are many recommended treatments but about 20% of patients continue to suffer whatever is done. Good cures usually surface quickly and the single most effective treatment appears to be a dental splint (orthotic) which separates the teeth somewhere between 1 to 8 millimetres. While the relief can be dramatic, and permanent the problems often return after a few weeks or months. This suggests to me that the splint may rest the joint in the short-term but the underlying cause remains. This explanation fits the fact that thickening the splint often provides a further period of relief but again the problem returns. Splints can also have side effects such as intruding teeth and despite what is done 20% or so of patients continue to suffer.
Other cures exist such as physiotherapy which can be almost as effective as splints, but again they seem ineffective for about 20% of patients. A number of clinicians and patients consider changes in the content and consistency of our diet is important, but ‘cures’ on this basis are rather unspecific and it not appear to have a high ratio of success.
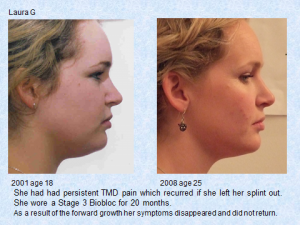
With orthotropics we try to reverse the life-style changes because we believe that modern living has encouraged many children to leave their mouths open and also to swallow with their tongue between their teeth. Research shows that this is a major reason for both jaws failing to grow forward which in turn disrupts the way the teeth and jaws meet and effects the position and form of the TMJ. Orthotropic treatment is based on the ‘Tropic Premise’ which says “correct oral posture is with the tongue resting against the palate, the lips sealed and the teeth in light contact for about six hours a day”. Orthotropic treatment aims to train children to keep their mouths closed which increases forward growth improving the teeth and face. This seems to reduce their susceptibility to TMJ problems later but is only fully effective with growing children. However adopting the Tropic Premise can often cure TMD pain in young adults possibly reaching that last 20%. see the picture below.