History
Over the last 100 years the consensus of professional opinion, in regard to extracting teeth has swung from almost never extracting teeth to almost always extracting teeth and halfway back with possibly a more mixed standpoint in today’s more diverse and international society. At each swing practitioners holding the opposing view were considered outcasts. Current opinions vary between countries and ideologies. Most patients would be surprised at the polarization, even animosity, between these groups and it is unfortunate that little open scientific debate occurs between them.
Philosophical overview
It has been assumed for most of the existence of orthodontic practice that malocclusion (crooked teeth) is an entirely genetic condition. You are born with either too many, too few or the right number of teeth to fill the dental arches. Without good scientific data this assumption has persisted relatively unchallenged. Philosophical reasoning for extracting teeth was that if there were too many teeth to fit them some would need removing. Once all the adult teeth have arrived in the mouth, between 12 and 14 years of age, an assessment could be made whether to extract teeth or not.
Interestingly little general reasoning was made and the fact that no vertebrates exist with additional teeth to requirements and that none of our ancestors had additional teeth was overlooked. Only 1000 years ago in Scandinavia several studies reported that all the skulls examined had a full compliment of teeth present and correctly aligned, including the wisdom teeth and showed no signs of additional teeth.
Alternatives to orthodontic extraction
Many alternatives to extracting teeth have been put forward and some are currently used in orthodontic treatment:
Distalizing upper molars-
Pushing the upper molars teeth backwards makes space for the front teeth, using appliances such as the distal jet and headgear. This is an effective method of creating space on the front of the mouth but teeth are still lost at the back of the dental arch near the hinge which tends to magnify the tendency to facial lengthening.
Slimming teeth-
Teeth can be ground on both sides to create more space in mild to moderate cases of crowding allowing space for the remaining teeth to be aligned. Natural slimming of the teeth as they move against each other, known as Attrition, is a normal process and it is estimated by some that the native Australians lost the equivalent of a whole tooth width during their lifetimes.
Tooth slimming is often recommended when there is a little crowding in the lower arch while the teeth in the upper arch are well aligned in a situation known as a Bolton discrepancy.
Expansion
Widening the dental arches laterally (sideways) can also provide additional space, however unless tongue position is affected to maintain this expansion it is often unstable.
Who extracts the teeth?
In most countries the orthodontist will refer a patient back to the general dentist who will undertake the extractions. This may be done by an oral surgeon who is a specialist, trained to extract teeth, especially if the extraction is predicted to be difficult or the patient is compromised medically. General dentists with experience in Orthodontics will often extract the teeth themselves.
Which teeth are extracted?
Common adage in orthodontics is that you must extract closest to where the space is required, also aesthetically you should avoid extracting any of the front six teeth, the incisors or canines. This has made tooth number 4, the first permanent premolar (first bicuspid) the most common tooth to be extracted. At the height of the extraction philosophy the phrase “all fours on the floor” was a common nickname for this approach, when it was often felt wise to extract teeth in cases where there was no crowding, to prevent future crowding.
Some orthodontists concerned about the “dishing in” aspect of facial damage have taught to extract the tooth number five, the second permanent premolar (second bicuspid). Although it is more difficult to close the spaces, the extraction of tooth number six (the first permanent molar) or even seven (the second permanent molar) have also been advocated and in mild cases a single lower single incisor may be removed. The choice of extraction is also determined by the prognosis (health) of individual teeth and those with large fillings (especially if with root fillings) should be extracted in preference to perfectly healthy teeth, where possible.
Should teeth be removed for orthodontics?
Few areas within orthodontics (and possibly in dentistry) seem to have caused as much passion and polarization of viewpoints. This argument has raged since before “The extraction debate of 1911”. Careers have been made, reputations been dashed and there is still no consensus within the profession. The current view within the “Establishment” including the most teaching hospitals and the majority of Orthodontists trained within them is that; in some cases extractions are certainly required and in others they are unnecessary and when the correct decision is made there are few if any adverse side effects. Standing back a little from the details of this argument it has been noted that until recently none of our ancestors for 220,000 years, nor their ancestors for millennia, nor for that matter any of the other mammals through history have had extra teeth that require extracting. However currently a significant proportion of children in modern societies present to the orthodontist without sufficient space for all their teeth and extracting is often the simplest and most expedient approach, usually without any noticeable or immediate side effects or facial damage. Many individuals live a long and healthy life, with permanently well aligned dental arches having had extractions. Despite the numbers who eschew extractions this argument cannot be claimed to be clear-cut by either side.
Side effects of extractions in orthodontics- I
The debate against extractions in orthodontics has long been based around the supposed side effects of extractions. There are five traditional effects of extractions that have been proposed and denied without a clear consensus:
Dark corridors: When some individuals smile a dark space is present either side of their dental arches, between the white teeth and the outer corner of the lips. It is suggested that this is created or increased by orthodontic extractions that reduce and narrow the dental arches. The research undertaken by the “Establishment” suggests this is untrue, but this is criticised since it excludes unsuccessful cases. Case studies show evidence both to support and disprove this belief.
Reopening of extraction sites: The stability of orthodontics is discussed elsewhere (orthodontic stability) however one particular concern is that spaces sometimes open up where teeth were extracted. The spaces tend to be smaller than a single tooth suggesting that some slimming might have been a better treatment plan.
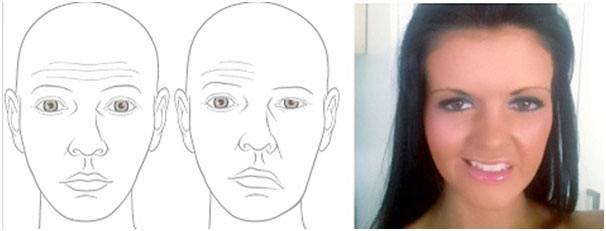
Aesthetic line and lip position: By considering the dental arches in isolation, contemporary orthodontics has focused on the effect of extractions on the support of the lips, but may have missed the larger picture. In there is crowding, aligning the teeth without extractions will require an arch of greater circumference, expanding the teeth either side and pushing them forwards at the front, pushing the lips forward. The opposite is true when extracting teeth and reducing lip support allowing them to flatten. In orthodontic assessment of the face the aesthetic line is drawn from the front bulbosity of the chin to a point, halfway between tip of the nose and its base where is meets the upper lip. This is known as Rickett’s E-Line and it is against this that an assessment of the lips are made and it is a simple exercise to make this assessment. If a friend holds a camera taking a profile shot while a ruler is held in this position both lips should be approximately on this line. Some reasonably good quality research has been done this area. It would appear that problems do occur but are due to a poor treatment plan of extractions. Good treatment planning can correct protrusive lips and avoid collapse when the lips are normal. Unfortunately this ignores the vertical effect of orthodontics and the loss of bone supporting the roots of the teeth.
Nasiolabial angle: In orthodontic assessment an angle is drawn at the intersection of the flat section of the upper lip and a flat section at the base of the nose, referred to as the nasolabial angle. The normal range appears to be approximately 90° to 120°, with a modern average somewhere between 95° and 100°. This angle can increase dramatically and look aesthetically displeasing when unnecessary extractions are performed pulling back the upper lip.
Side effects of extractions in orthodontics- II
In addition to the five traditional insights into facial damage, in orthodontic therapy there are two that do not seem to have been greatly recognised or given much consideration within orthodontic literature.
Facial support from teeth: Anecdotally it has been suggested that the bone surrounding the roots of the upper teeth, in particular, is lost after the removal of these teeth. This suggestion lacks quality research however some case reports appear to show a relationship.
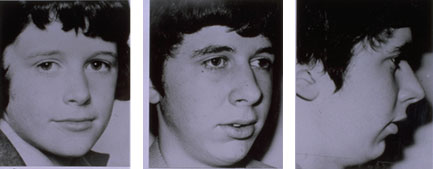
Facial lengthening: One of the most consistent observations of orthodontic treatment is that the anterior facial skeleton (the mid-third of the face) lengthens during orthodontic therapy, usually following fixed appliance therapy, retractive headgear, class 2 elastics and any distalizing therapy. This appears to be true in almost every single controlled research paper on the subject and is possibly one of the most consistent finding within orthodontic literature. It has also been observed that in general, facial lengthening is unattractive. From an Orthotropic perspective this is worsening the underlying problem while treating the symptoms. Although this observation has not become a widespread topic of interest, it has caused much deliberation for a few notable authors. A. Lundström and D. G. Woodside noted that there was not a single incidence of late mandibular growth in the Bulington growth study and suggested that “Horizontal increments of mandibular growth are usually seen following orthodontic treatment which has retracted the maxilla, and this probably represents a recovery from a downward and backward mandibular rotation created during the treatment.“ Individual variation in growth directions expressed at the chin and the midface Eur J Orthod (1980) 2 (2): 65-79 and Birte Melsen has written extensively on the loss of vertical control even appearing on national television to suggest headgear use should be banned, (Effect of cervical anchorage studied by the implant method EOJ 29 (2007) i102–i106) showing a dramatic increase in facial height for some individuals.
It is not fully understood what is causing this process however the suggested causes of facial lengthening are:
Conning: once the brackets had been placed on each tooth a thin arch wire usually made of nickel titanium is placed, running through all the brackets that works to level and align the dental arch. The arch wire will be bent so that it can engage into each bracket. This sets up a force that aims to push the brackets (and the teeth attached to them) into alignment. This is the main principle of fixed appliance orthodontic therapy. This first phase known as “leveling and aligning” produces some of the largest movements of teeth with some very complex mechanical interrelationships (statically indeterminate force systems) between the teeth. The teeth, especially the root tips, move in a very unpredictable pattern often round tripping (making a circular movement to return to the original position- often due to the movement of another tooth close by). All the sideways (lateral) forces are reciprocated by other sideways movements and are cancelled out, however the vertical forces must be reciprocated by the biting forces, muscle tone and it is often the very individuals without these that have the most crooked teeth. In addition to this, since teeth naturally erupt and naturally resist intrusion (pushing into the bone) the net result of this first phase of orthodontics is to vertically erupt the teeth lengthening the anterior facial height.
Sensitive teeth: The process by which a tooth moves through the bone due to fixed appliances is quite remarkable, part of the process is a chronic inflammatory reaction that removes the preceding bone before new bone is formed behind the teeth. As with all chronic inflammatory processes, this can be a painful process and during movement the teeth tend to be sensitive to bite on. Due to this the biting forces and resting muscle tone tends to be reduced, thus lengthening the face, as discussed in the section on “Causes of crooked teeth”.
Damage to oral posture: Any appliance that occupies space within the oral cavity can affect the postural and functional position of the soft tissues such as the tongue and lips. The work of Harvold in his monkey experiments (Primate experiments on oral sensation and dental malocclusions, AJO Volume 63, Issue 5, May 1973, Pages 494–508) shows how simply placing a piece of plastic in the palate can have a dramatic effect on the direction of growth of the face. Fixed appliances by their nature seem to damage the natural lip seal and large braces in the roof of the mouth such as hyrax, quad helix or bulky removable appliance often damage the resting tongue position, thus worsening the underlying problem.
Direct affects on the position of the maxilla or mandible: Retraction headgear (the traditional type that pulls backwards) and class II elastics (the ones in the mouth that fit onto fixed braces to encourage the lower jaw to grow forwards) both tend to pull the upper jaw back and down, lengthening the anterior facial height. In addition bite raising appliances lengthen the resting muscle length of the face, once lengthened at this sensitive age there is a good chance that the effect will be permanent. Research consistently suggests that all of these appliances seem particularly consistent in increasing facial height especially for the individuals where this is not desired.
The effect of facial lengthening is often known as “unfavourable facial growth” and it is suggested that this is a natural genetic response rather than an effect of orthodontic treatment. There is little good evidence to support either argument however circumstantial evidence would suggest that this is the effect of most orthodontic treatment.
Responsibility of the general dentist
Although the general dentist extracts teeth under prescription from the orthodontist, responsibility tends to live with the individual who undertakes an action. As such it has been suggested that general dentists may share joint liability for problems associated with extractions for Orthodontic reasons. Sensible advice for general dental practitioners would be to check the treatment plan with the orthodontist, confirm that the side effects outlined have been reasonably considered and finally to take some quality lateral and facial photographs prior to commencing the treatment. (see Orthodontic outrage, info for dentist).