May 22,2020
Precis. Diagnosis for orthotropics is very different from orthodontics. You are measuring the shape of the face and deciding what has caused any unattractive features. An orthotropist needs to learn how to recognise poor development and decide on the best way to correct it which is almost always to encourage forward growth of the Maxilla and Mandible.
Lecture 6. Diagnosis for orthotropics is very different from orthodontics. With a young patient the orthotropist is not very concerned with the position of the jaws or teeth because these can easily be changed. The posture of the mandible and tongue is of far more concern. Many orthodontists criticise orthotropists for sloppy diagnosis but the clinician only needs to note the position of the jaws so he can estimate how long it will take to re-position them. The position of the teeth is of less concern as their correction will depend primarily on the age and the co-operation of the patient.
I can usually diagnose the problem as the patient walks into the room and have judged what will be needed before they have sat down. I say that to draw attention to the simplicity of diagnosis. Apart from the 4% of genetic deformities such as a cleft lip, which are usually very obvious, all malocclusion is due to poor oral posture. There are just three things you need to look at their jaw, lips and tongue. You can then measure how far they are from the ideal and decide the extent to which you can restore it, knowing that a full correction is rare over the age of six.
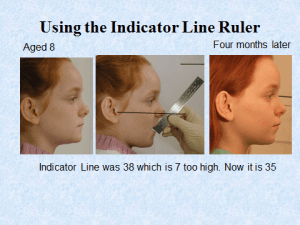
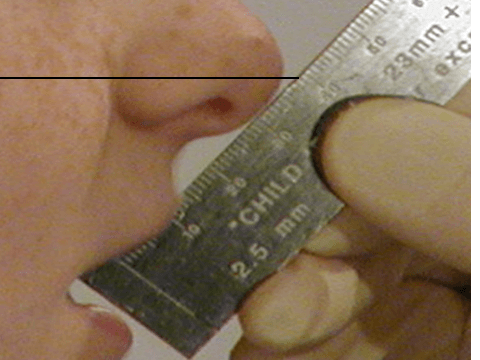
The first and most basic measurement is the Indicator Line. This is simply the distance between the tip of the nose to the incisal edge of the upper incisors. It can be measured with an indicator line ruler, obtainable from www.johnmeworthotropics.co.uk . It is a way of measuring how far back and down the maxilla and incisors are from the ideal. It only gives an ‘indication’ but this has proved a simple and surprisingly accurate way of assessing the severity of any malocclusion. It should be about 28mm at the age of five and increase 1mm per year until puberty when it should be 38 for a man and 36 for a girl. (see picture below)
There is also a lower Indicator line measured between the incisor tip and the soft tissue vertically below it. It is suggested that this should be 2mm less than the upper Indicator Line. It is very rare to find someone with correct Indicator Lines, but it is also very rare to find anyone with room for 32 teeth with 10mm of spare space behind the wisdom teeth. They are usually the same people.
One needs to assess the shape of the face and especially the slope of the forehead to understand the head posture and growth direction (See illustration).

Also record the postural features such as how much the lips are apart. To do this I ask the patient to count up to six and watch the average separation. A natural seal is rare and research suggests that healthy 4 to 5 year old children in developed countries, leave their mouth open more than 80% of the time (Glatz-Noll,E & Berg,R. 1991).
In some groups with bi-maxillary protrusion the mouth can be open 15 to 20mm. There are many other postural features which can be recorded relating to various muscle bulges, which indicate para-functional activity. The most important records are facial photographs from the front and side. Three-quarter views are also useful for showing Maxillary change (see illustration). For record purposes these should be taken with a 5cm marker or ruler in the sagittal plane so that subsequent growth can be measured.
I may take X-rays of the teeth, but I do not find lateral skull X-rays helpful for forecasting growth or even of much use for recording changes. We will talk later about measuring growth and growth direction with a Gnathiometer.
John Mew has been working on a lecture series going into more depth on his thoughts, ideas and what inspired them. In this episode he talks about diagnosis of the face.
If there are any other topics you want us to cover please let us know. Engage with Prof John Mew or Dr Mike Mew on this topic; Professionals (of any medical/health discipline);
https://www.facebook.com/groups/Ortho… or https://www.facebook.com/groups/Ortho…
Non Professionals;
https://www.facebook.com/groups/crani…
https://www.facebook.com/groups/crani…
To see the text version please visit;
https://orthotropics.com/john-mews-le…
Please consider joining our Patreon Community:
https://www.patreon.com/orthotropics
Particularly if you have;
1) gained any benefit from the information that we have provided (usually for free).
2) wish to have the benefits of being a patreon member.
3) believe in, and wish to support our mission to gain full, free and fair debate (engagement) on these issues within the orthodontic and dental community.