
Nov 03,2020
Orthotropics 13. Contrasting Orthodontic Concepts.
Precis. Most dental and orthodontic students attend university to learn how to treat patients, so they inevitably learn past methods. Some will stay with these all their life, others will change their ideas; maybe more than once. For many it has not been until near the end of their careers that experience teaches them that retracting ‘sticking out’ front truth may not improve appearance.
Lecture 13. Time does not always improve our knowledge. As I said in my first lecture, Edward Angle stated “Orthodontic treatments are very unlikely to succeed, if the functional disorders are still going on”. Charles Tweed one of his more radical students suggested four premolars should be extracted and this concept was adopted by most orthodontists for the next 60 years. However at the end of his career Tweed said “in future the vast majority of orthodontic treatment will be carried out during the mixed dentition”. So ultimately both of them adopted concepts very similar to my own.
By the time many of us have realised the true nature of malocclusion it is too late to create a new paradigm. Today many orthodontists around the world still strive for perfectly straight teeth probably because they are all dentists. I was taught “if you treat correctly the teeth will stay straight, if they don’t, you have not done it correctly”, but now it is accepted that we have to retain the teeth for the rest of a patient’s life. Is this inevitable and are the patients getting a fair deal?
The constant theme of this lecture series is facial appearance. In lecture 6 I described the ‘Indicator Line’ which I created in the 1970s to measure facial lengthening. It relates closely to facial attractiveness as well as malocclusion but I found that the Indicator Line almost always increased when fixed appliances were used, especially if this was coupled with extractions.
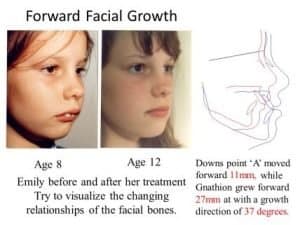
It was the Indicator Line that first convinced me that “sticking out incisors” are actually too far back and the rest of the face is even further back. See the illustration of an eight year old girl with a 14mm overjet. I proclined the incisors to reduce the Indicator Line which increased the overjet to 17mms before encouraging the rest of her face to grow forward. As a result her chin, the Gnathion came forward 27mm.
That was 50 years ago and I find it hard to believe that orthodontists are still retracting “sticking out” incisors. Even more concerning, few orthodontists appreciate the consequences of this. It routinely retracts the maxilla and mandible which not only spoils the face but reduces the arch length, therefore leaving less room for the teeth. Sadly this worsens Sleep Apnoea and Temporomandibular problems which are both related to retruded jaws, as well as many ear nose and throat issues. This is because none of the accepted treatments are able to make the mandible grow forward, so the maxilla is pulled back instead.
Many clinicians use ‘Functional’ appliances to bring forward the mandible in class II cases and the Twin Block is one of the most popular appliances in the world. However my experience is that these appliances only achieve one or two millimetres of forward growth and the rest of the overjet is corrected by facial lengthening and upper dental retraction with lower proclination.
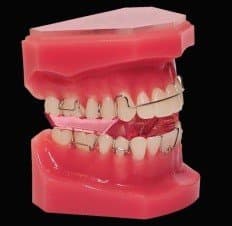


Recently positioners such as Invisaline and Smile Direct have become popular, mainly because they are less work and therefore less expense. They usually align the teeth in class 1 cases very nicely as you can see, but are not so easy for class II or III cases. Frequently they lengthen the face, because the patient starts to swallow with their tongue between their teeth as can be seen here. Some cases lose lateral control while others Tip, Roll or Yaw. All these problems are difficult for orthodontics to control, although fairly easy for an Orthotropist.
As a general rule neither Prof or Dr Mew have time to engage in the comments section, their focus must be to gain as much real change and scientific engagement as possible, and this would otherwise consume all their time. If you want to engage with Prof John Mew or Dr Mike Mew on this or other topics then follow these links (if you want a personal opinion on your situation then please book an on-line consultation at https://orthodontichealth.co.uk/book-…
Professionals (of any medical/health discipline); https://www.facebook.com/groups/Ortho… or https://www.facebook.com/groups/Ortho…
Non Professionals; https://www.facebook.com/groups/crani… or https://www.facebook.com/groups/crani…
For more general information please visit; https://orthotropics.suryawebsolution.com.np/
Please consider joining our Patreon Community: https://www.patreon.com/orthotropics Particularly if you have; 1) gained any benefit from the information that we have provided (usually for free). 2) wish to have the benefits of being a patreon member. 3) believe in, and wish to support our mission to gain full, free and fair debate (engagement) on these issues within the orthodontic and dental community.