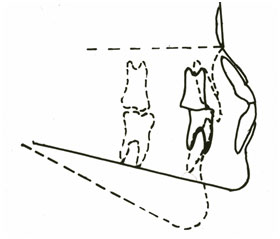
Within this site are several well-supported texts discussing how external influences in the modern environment are leading to a lengthening of the anterior facial skeleton. This is well illustrated if you compare the tracing of a primitive skull shape with a modern average such as is used by orthodontists when they are planning treatment (see below). The reduction in the muscular effort and a lowering of the tongue from its habitual position on the roof of the mouth have effected a large change in anterior facial skeleton.
 |
|
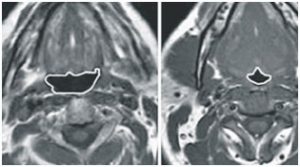
As the craniofacial complex lengthens, the mandible hinges back and downwards carrying the tongue down into the airway. If a face is longer it is going to be narrower and shorter, reducing the cross sectional area. This area contains the tongue, teeth and airway and if there isn’t space for the teeth then your airway is at serious risk. The most statistically significant single measurement in the diagnosis of sleep apnoea is the distance from the insertion of genioglossus (just behind the chin point) to the hyoid bone (the Adams apple), which is more significant that obesity and body mass index. The more the mandible hinges back the smaller this area becomes.
 |
|
 |
When awake, we usually make two subconscious postural adjustments to cope with this situation. One is to extend the head and neck, opening the airway in a similar manner to the tipping the head back for Cardiopulmonary Resuscitation (CPR) or when giving an anaesthetic, the other is to move the mandible and tongue, for example lowering the mandible slightly while the tongue is held a little forwards, moving some of the bulk of the tongue forwards out of the airway. It is also possible to increase the motor tone of the muscle in the airway and those holding the base of the tongue. Such compensatory functions can be very effective at maintaining a patient airway, however they take a level of conscious command that is inevitably reduced during sleep, when the tongue falls back into the airway causing nocturnal sleep apnoea which is exacerbated by sleeping face upwards.
The next time you travel to a busy public environment such as a shopping mall, restaurant or school observe how people hold their mouths at rest. Observe if you can draw any conclusions between how much their mouths are left open and how they look, or rather the shape of their faces. This is especially apparent in children under puberty as they have yet to gain such a strong social awareness so are not trying to conform to any social pressures and when they are fully relaxed at home watching something that fully engages their consciousness. The next time you are in a movie theatre look backward at all the staring faces fixated on the screen, compare the faces with their mouth closed with those that are really open. The conclusion could not be more dramatic, people who hang their mouths open, really don’t look so good, and you don’t have to be a scientist to work that out.
 |
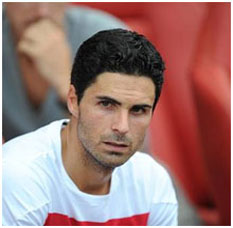 |
| Mouth always closed, or almost closed- good cheekbones, excellent face shape | Mouth slightly open- lower cheekbones |

To move the mandible and tongue, for example lowering the mandible slightly while the tongue is held a little forwards, moving some of the bulk of the tongue forwards out of the airway. It is also possible to increase the motor tone of the muscle in the airway and those holding the base of the tongue. Such compensatory functions can be very effective at maintaining a patient airway, however they take a level of conscious command that is inevitably reduced during sleep, where the tongue then falls back into the airway causing nocturnal sleep apnoea which is exacerbated by sleeping face upwards.
The systemic effects of sleep apnoea cannot be understated, it has been suggested that it is involved in the pathogenesis of heart disease, Attention Deficit Hyperactivity Disorder (ADHD) and even obesity (which suggests a pathological vicious circle may exist).